When Your Child Has Clubfoot
Your child was born with clubfoot. This is a problem with the shape of the foot (deformity). The foot is hooked and turned inward, with the side or the top of the foot pointing down. It is because of shortened tendons in the foot and lower leg. Clubfoot is congenital, meaning your child was born with it. It may affect one or both feet. Clubfoot is painless and very treatable in infants.
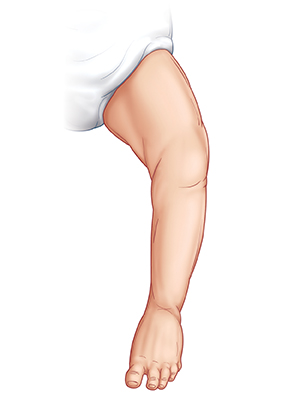 |
| Normal foot. |
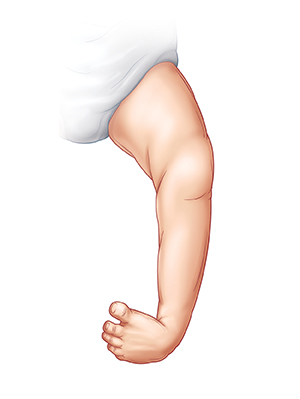 |
| Clubfoot. |
What causes clubfoot?
The cause is not fully known. Some things we do know are:
-
Clubfoot can run in families.
-
More boys than girls are born with clubfoot.
-
A child with nervous system problems such as cerebral palsy may be more likely to have clubfoot. But a child with clubfoot is not more likely to have nervous system problems.
-
It occurs in both feet in 1 in 3 cases.
-
In 1 in 10 cases, the child has another related problem.
How is clubfoot diagnosed?
Clubfoot is easily diagnosed by looking at the foot when the child is born.
How is clubfoot treated?
Clubfoot is very treatable if the treatment plan is followed. The goals of treatment are to make the child’s foot look normal, move in a normal way, and be comfortable to walk on. For treatment, the child is likely to be referred to a pediatric orthopedist. This is a healthcare provider specializing in treating bone and joint problems in children. Treatment options are outlined below.
-
Casting using the Ponseti method is the most common treatment in babies:
-
Ideally, casting begins in the first few weeks of life.
-
A series of 6 to 8 toe-to-groin casts are used. The casts are changed weekly at first, then every other week. By 3 months of age, casting may be complete.
-
Between casts, the healthcare provider moves and stretches the foot into a more normal position.
-
To maintain correction after casting is finished, the child wears shoes attached to a bar all the time for 3 months, then only at night for 2 to 4 years.
-
Other options may be used instead of, or in addition to, the Ponseti method. These options include moving and stretching the foot by hand, using short-leg casts, and using splints with adjustable adhesive straps on the child’s foot for periods of time.
-
Surgery may be done in children 4 to 5 months or older who have not been treated. Or it may be done if casting has not achieved full correction. The surgery releases a shortened tendon that is pulling on the foot. In some cases, the surgery may be more extensive.
What are the long-term concerns?
If clubfoot isn’t treated, a child can have difficulty walking and functioning normally. But if clubfoot is treated, many problems can be prevented. After treatment:
-
A child with clubfoot can wear regular shoes, run, jump, and be active. In fact, some children born with clubfoot have gone on to have professional athletic careers.
-
The child will have a foot and calf that are slightly smaller than the other foot and calf. This difference will never go away but rarely causes problems.
-
The child may have a small leg-length discrepancy (a leg shorter than the other). This is usually not a problem. Have the child checked regularly as they grow.
© 2000-2024 The StayWell Company, LLC. All rights reserved. This information is not intended as a substitute for professional medical care. Always follow your healthcare professional's instructions.